Darin Ingels, ND
SUmmary:
In the full presentation Lyme, Mold, and Mycotoxins: strategies for Navigating Complex Illness, Darin Ingels, ND, discusses the origin of Lyme Disease, how Lyme is spread, different ways to test for Lyme Disease and treat those affected by Lyme Disease.
Lyme Disease (LD) is among the more difficult of chronic syndromes – difficult to define, to diagnose and to treat. Since the mysterious outbreak of juvenile rheumatoid arthritis in the 1970s in Lyme, Connecticut, was first connected to microbial Borrelia burgdorferi spread by ticks, the understanding of these conditions has increased as Lyme itself has spread through the US and Europe.
Several species of ticks are expanding their range. The spread includes Canada, although Canada drastically underreports Lyme cases. Dr. Ingels provides considerable detail on Borrelia variants with maps documenting its relentless advance during the last few decades. He mentions that US variants have a stronger T-1 pro-inflammatory response, while European variants have a strong T-17 pro-inflammatory response.
Making identification of Lyme more difficult is the slow replication of Borrelia species (days instead of hours) and the organism’s ability to change shapes. The production of antibodies by Lyme sufferers isn’t dependable either. Many patients are entirely seronegative.
Laboratories often do not test for the full extent of the antibodies that have been associated with Lyme. The well-known bull’s-eye rash resulting from a tick bite is only present in 70% of patients according to the CDC, but other sources say 40%, and many Lyme sufferers have no recollection of a tick bite.
Symptoms are vague and overlap with other infectious and autoimmune conditions, which further confounds the problem of Lyme diagnosis. In children, confounding is even higher and symptoms include PANS and OCD. Also, diseases such as tularemia may present similarly to Lyme.
Dr. Ingels points out that the CDC criteria for Lyme Disease was designed for surveillance purposes and do not necessarily reflect active infection with Borrelia species. The official diagnosis of Lyme Disease is a clinical diagnosis (signs and symptoms). The CDC warns against diagnosis of asymptomatic individuals, although it is possible to carry the microbes without symptoms. CDC-approved testing includes ELISA and Western blot: these are 40-year-old criteria.
ILADS (the International Lyme and Associated Disease Society) has more complex criteria for diagnosis of Lyme (LD) and coinfections. Their LD assessment approach includes a symptom questionnaire and suggested labs include hormones (thyroid, adrenal), nutritional (Vitamin D, minerals, amino acids), and immune markers as well as microbial coinfections. However, different laboratory tests may report markers for different microbial strains.
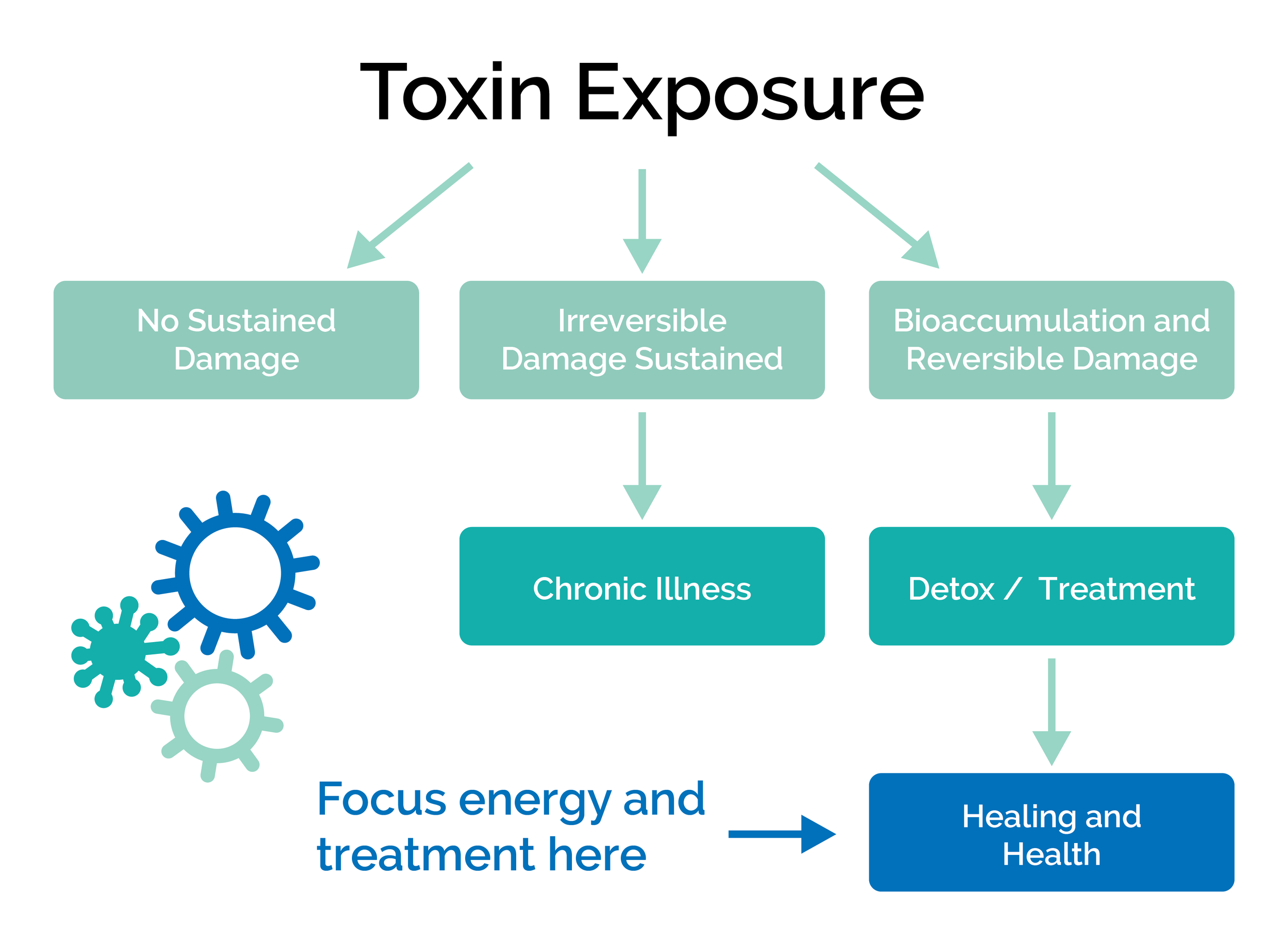
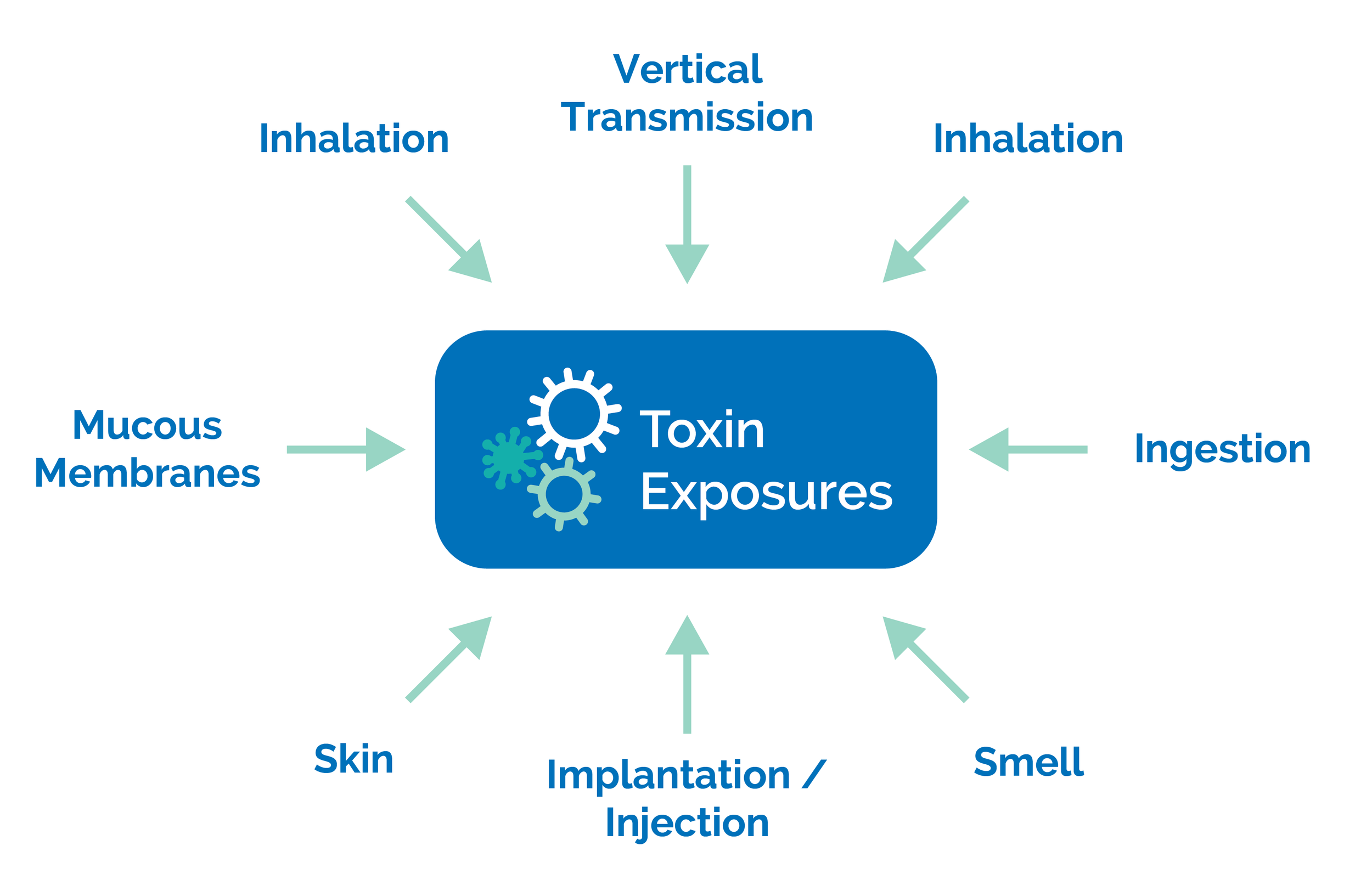
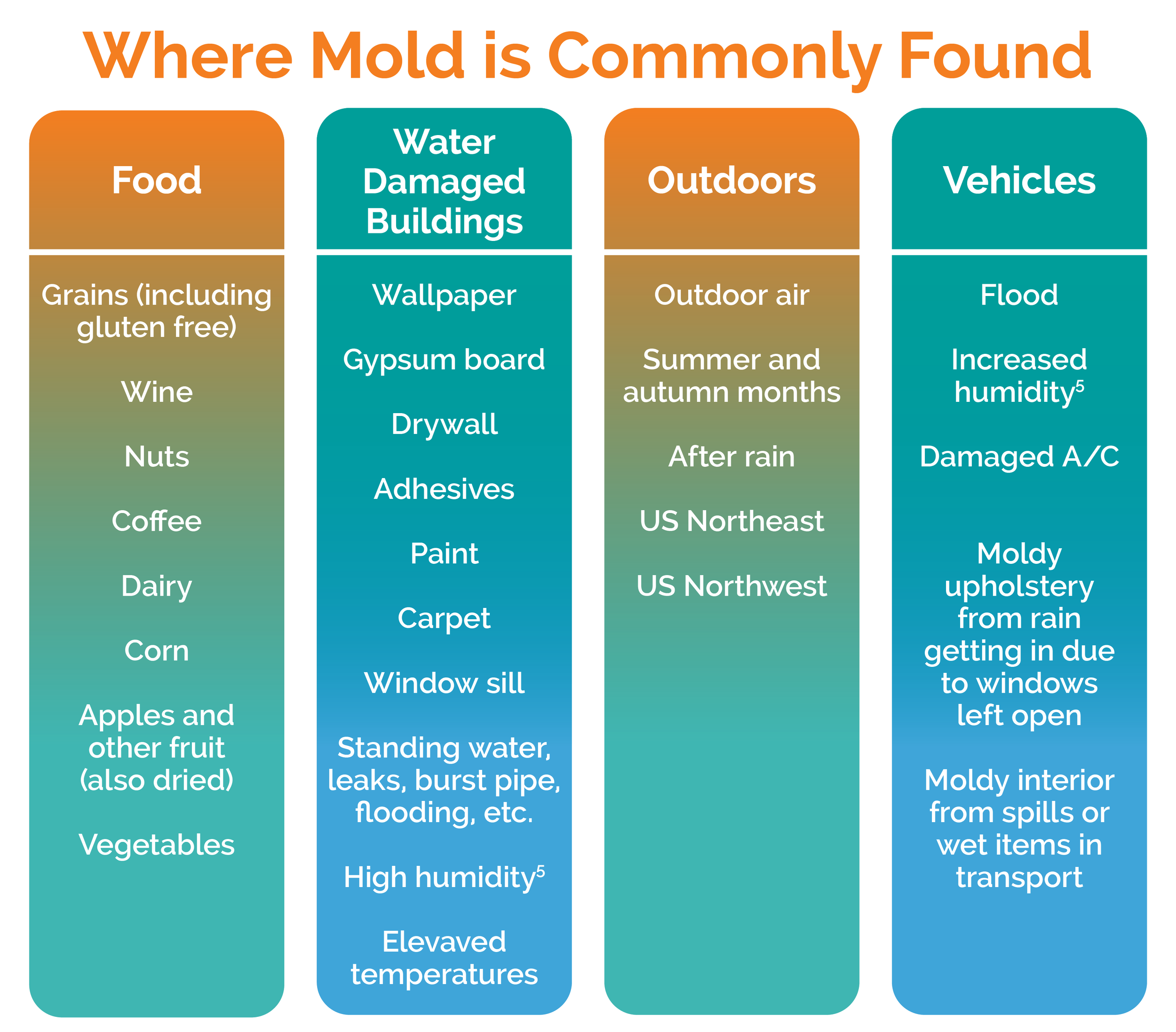
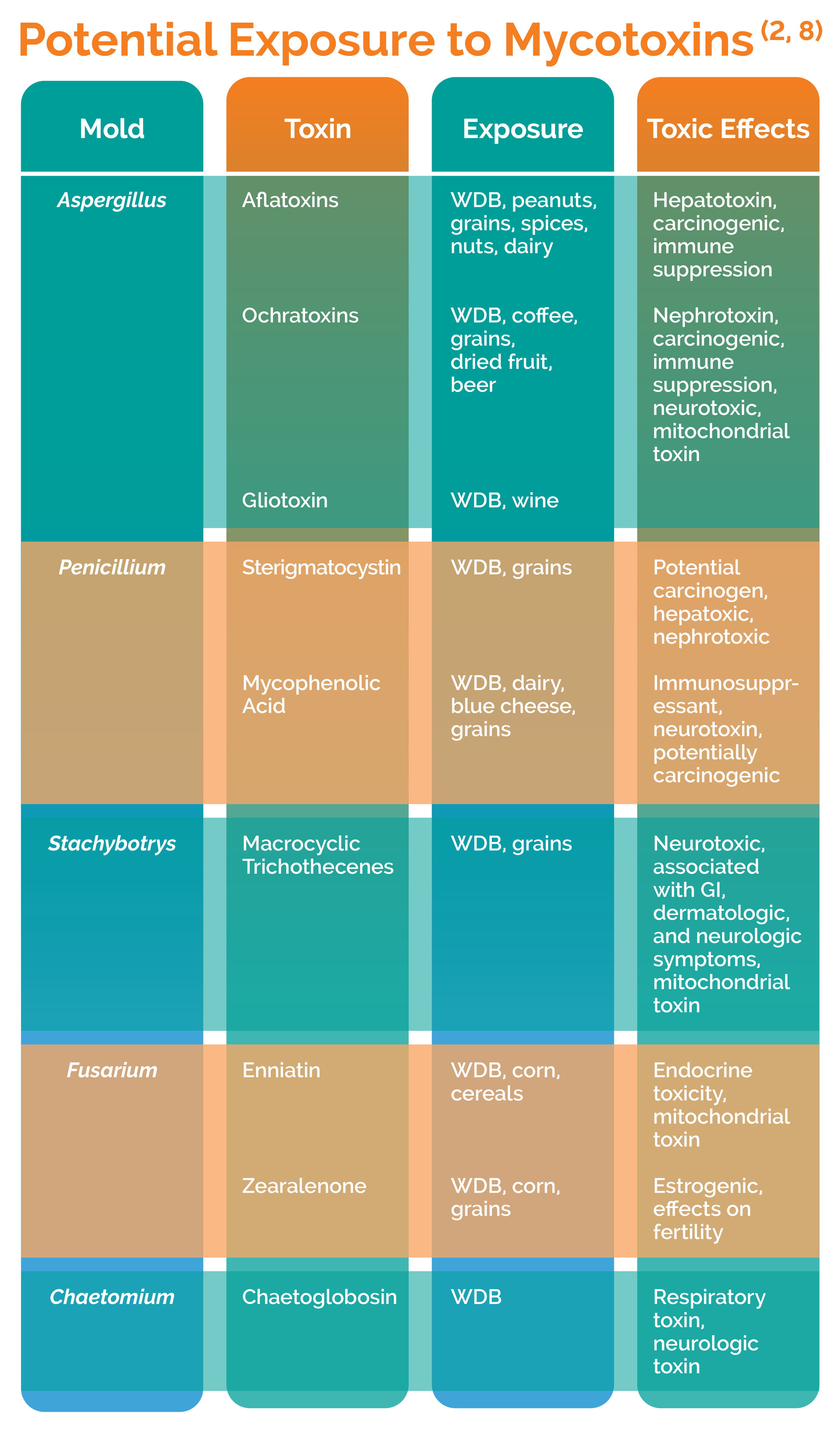
Dr. Ingels then segues into the involvement of mold as a major confounder of Lyme diagnosis. Mycotoxin toxic effects (mycotoxicosis) often overlap with Lyme Disease effects, and the damage both can do to the terrain also allows them to persist in a patient and contribute to ongoing oxidative stress and cell damage.
Fixing the terrain begins with – no surprise – healing the gut. Dr. Ingels offers the standard anti-inflammatory supplements such as probiotics and glutamine, and goes on to provide detailed diet guidance, emphasizing alkaline foods. The next step is to treat active infections, preferably with herbal supplements rather than antibiotics. He recommends several lesser-known herbal products for Lyme. Steps to reduce stress, improve sleep, and remove mold from the body and the environment are also presented. Treatment protocols should be tailored to each patient: “the best binder is the one your patient will take and tolerate’. Since sensitive mitochondria suffer “collateral damage” from these chronic conditions, Dr. Ingels winds up the lecture with mitochondria support supplements and detoxification strategies.

Order a Test or
Open an Account
GPL improves health treatment outcomes for chronic illnesses by providing the most accurate, reliable, and comprehensive biomedical analyses available.