We’re constantly exposed to mold when we’re outdoors even though we can’t see it. Our forecasters tell us it’s there and how much of it is in the air during the evening weather forecasts.
On days when the count is moderate to severe, we can see a rise in allergy-type symptoms in individuals with allergies.
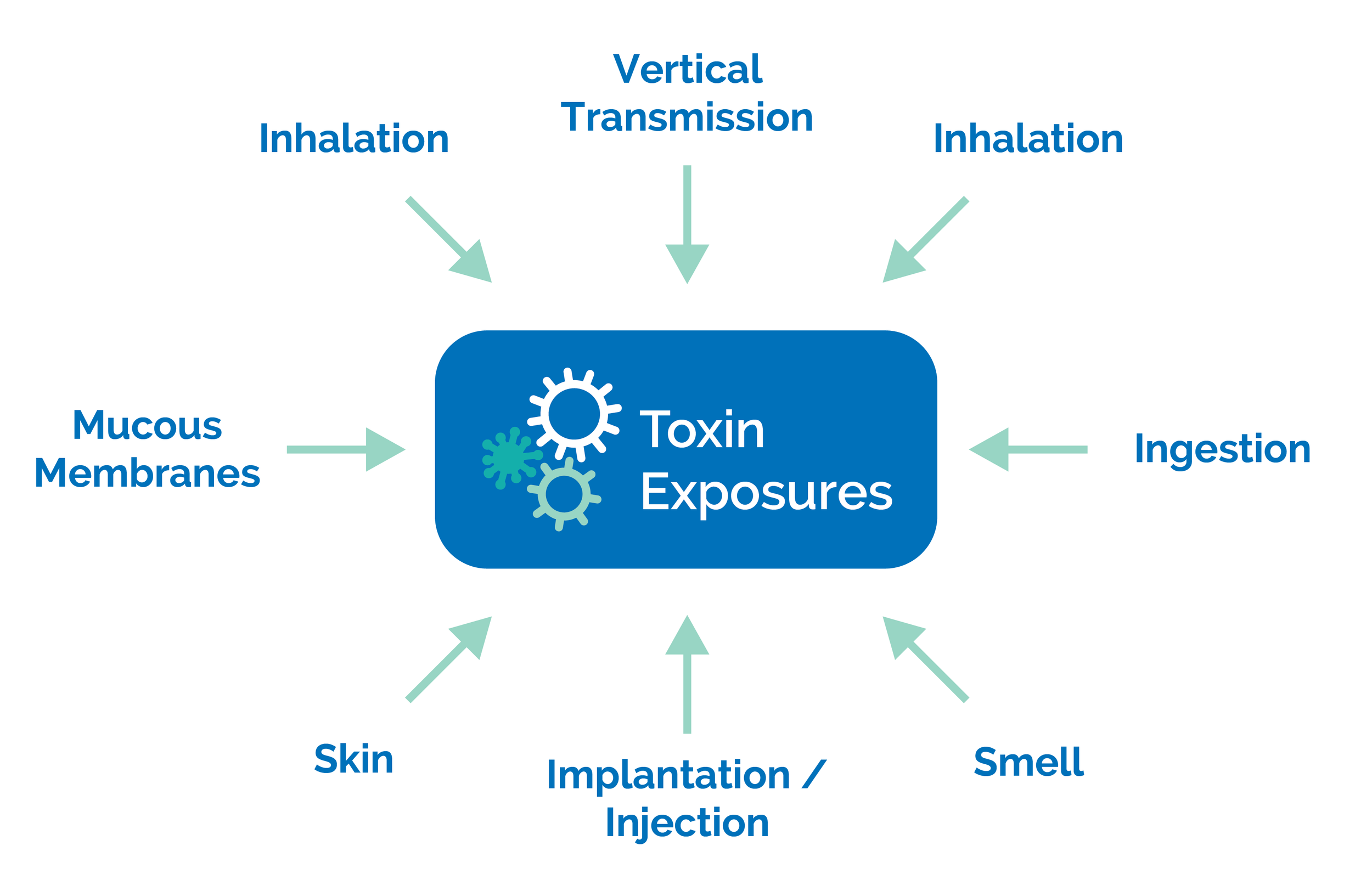
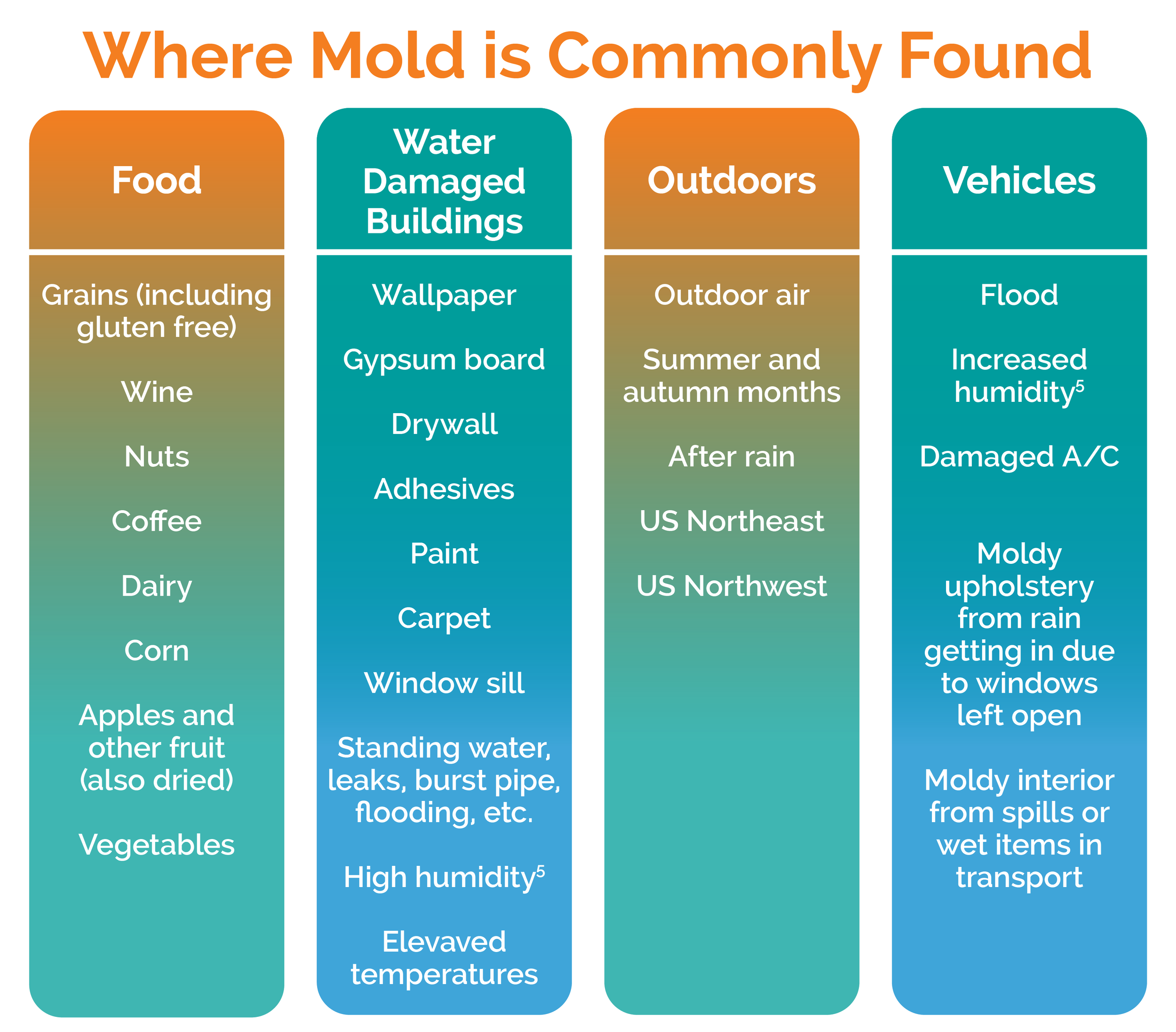
Another common source of mold exposure is from our diet. Certain foods are more prone to mold growth due to the way they are stored and/or grown. There are checks and balances that limit the number of mold/mycotoxins that are allowable before it is sent to market. This limits our exposure from food unless we overindulge in these foods. Common foods include coffee, grains, corn, dairy, wine, etc. Learn more about mold and mycotoxins in food here.
Mold decomposes dead organic matter so it can grow on wood, the paper facing on gypsum board (drywall) and other materials made from wood. To grow, mold requires oxygen, heat and moisture. Due to this, mold commonly contaminates water damaged buildings. Materials often found to be contaminated include wallpaper, gypsum board, adhesives, pastes, and paints(1,5).
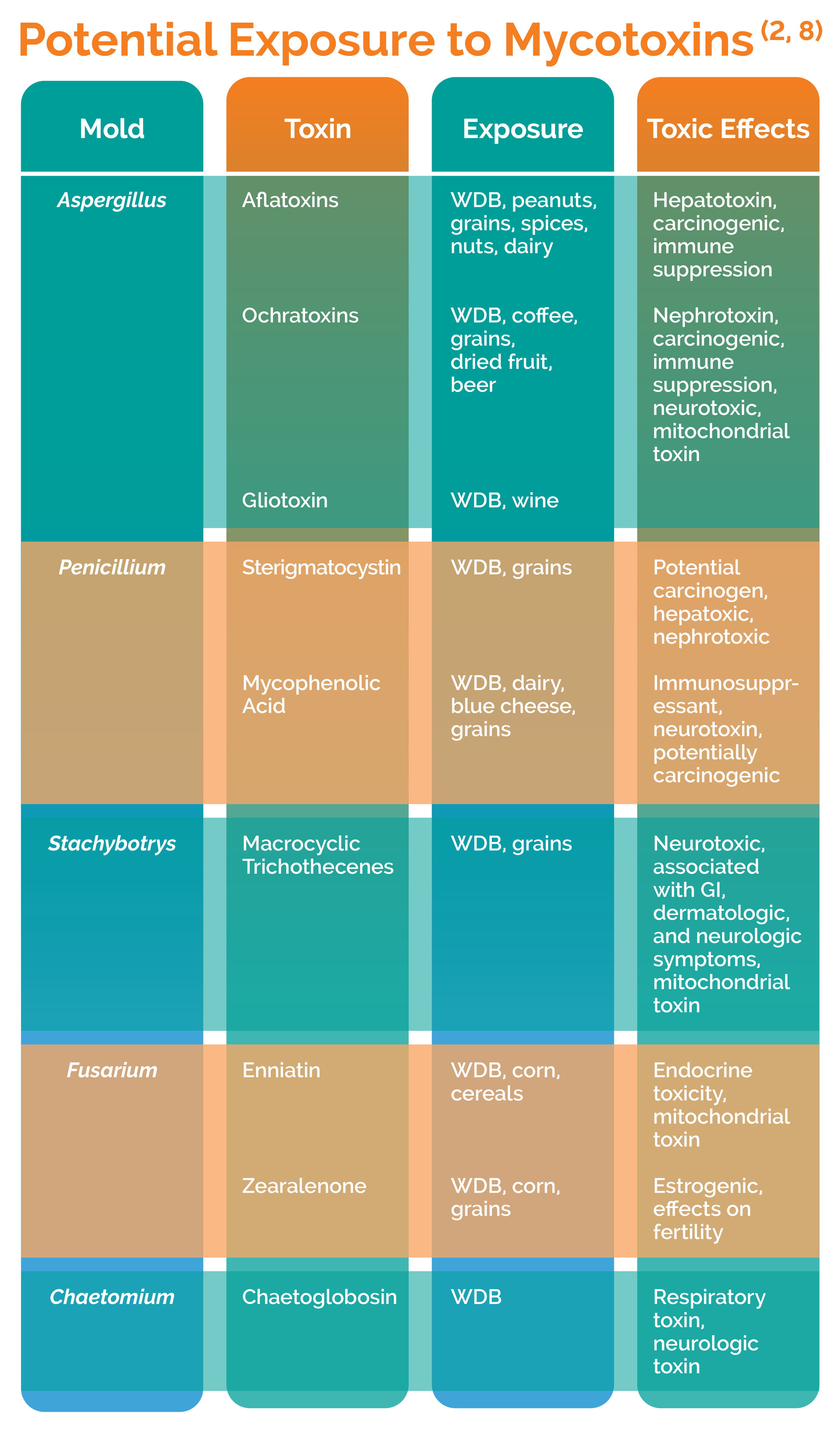
Although it doesn't grow on non-organic matter like concrete and glass and metal, the dirt on these materials when in the right environment will allow for the growth of mold (1). This is where people get overly exposed to mold and its mycotoxins. The most common are Penicillium chrysogenum, Aspergillus versicolor, and Chaetomium globosum (1).
When we get exposed to mold, we’ll either have no reaction, an allergic reaction, or a toxic reaction. In certain cases, we’ll experience both allergies and toxicity. So, what's the difference between an allergy and toxicity?
How the Body Fights Back From Mold Exposure
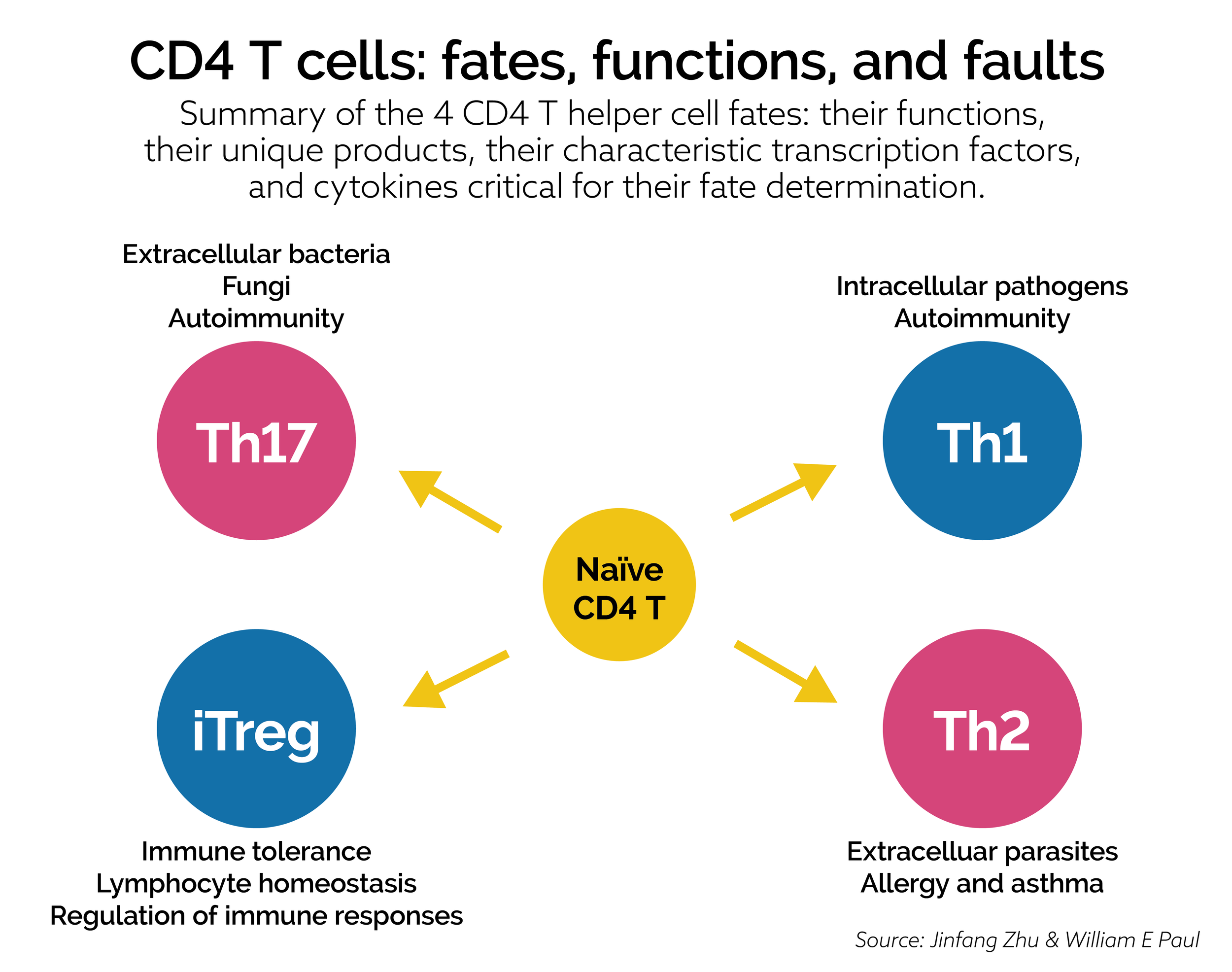
When an allergy is present, exposure to the offending substance or antigen triggers a response. This response is made by the immune system. In a true allergic situation, immunoglobulin E (IgE) antibodies are produced by the body. These IgE antibodies attack the antigen, in this case mold, and bind to cells like mast cells and basophils(7). This then triggers the release of chemical mediators like histamine. These chemicals are what induce the symptoms associated with allergies.
Allergic reactions can also happen to common household molds rather than just molds that produce mycotoxins in water damaged spaces. Commonly people experience itchy watery eyes, sneezing, coughing, urticaria, sinusitis, asthma and wheezing, etc.(7) In sensitive individuals, whenever exposed to the antigen these symptoms will arise.
During peak mold months in the summer and fall, you may be one of the millions of consumers combing your local drugstore for over-the-counter allergy medications and nasal sprays to find any relief from common allergens like pollen, and mold. You might also watch the weather forecast to prepare for the air quality and level of mold spore spikes in the air. If you’re unfortunate enough to live in a water-damaged building, you can expect to see a chronic persistence of these allergic type symptoms.
When Mold Exposure Elevates to a Chronic Illness
Mold toxicity is different from mold allergy. In a toxicity, there is an over exposure to toxic metabolites that are produced by mold organisms. Toxicity states do not require immune mediated responses to be harmful or to cause what is experienced by the affected party.
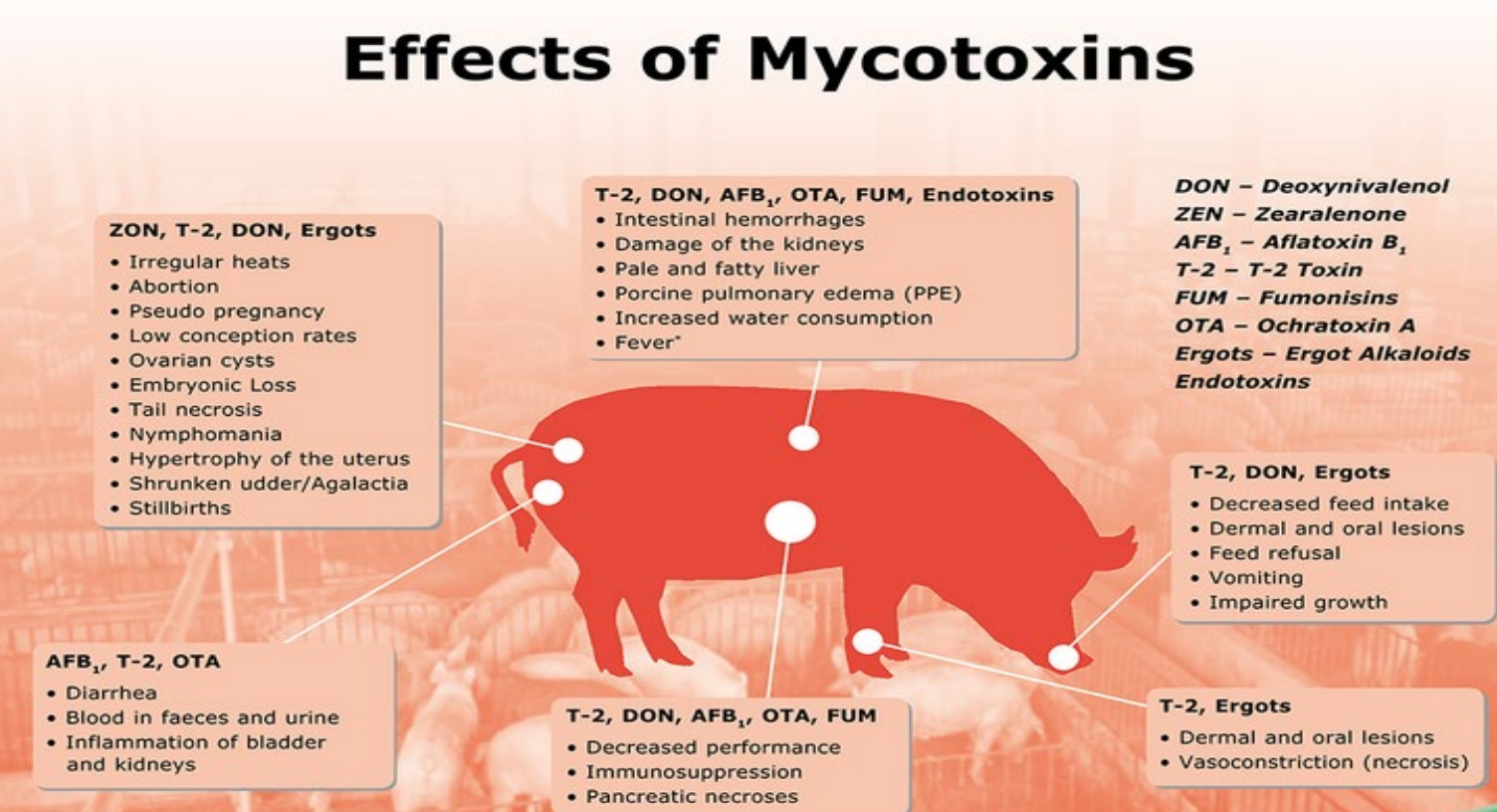
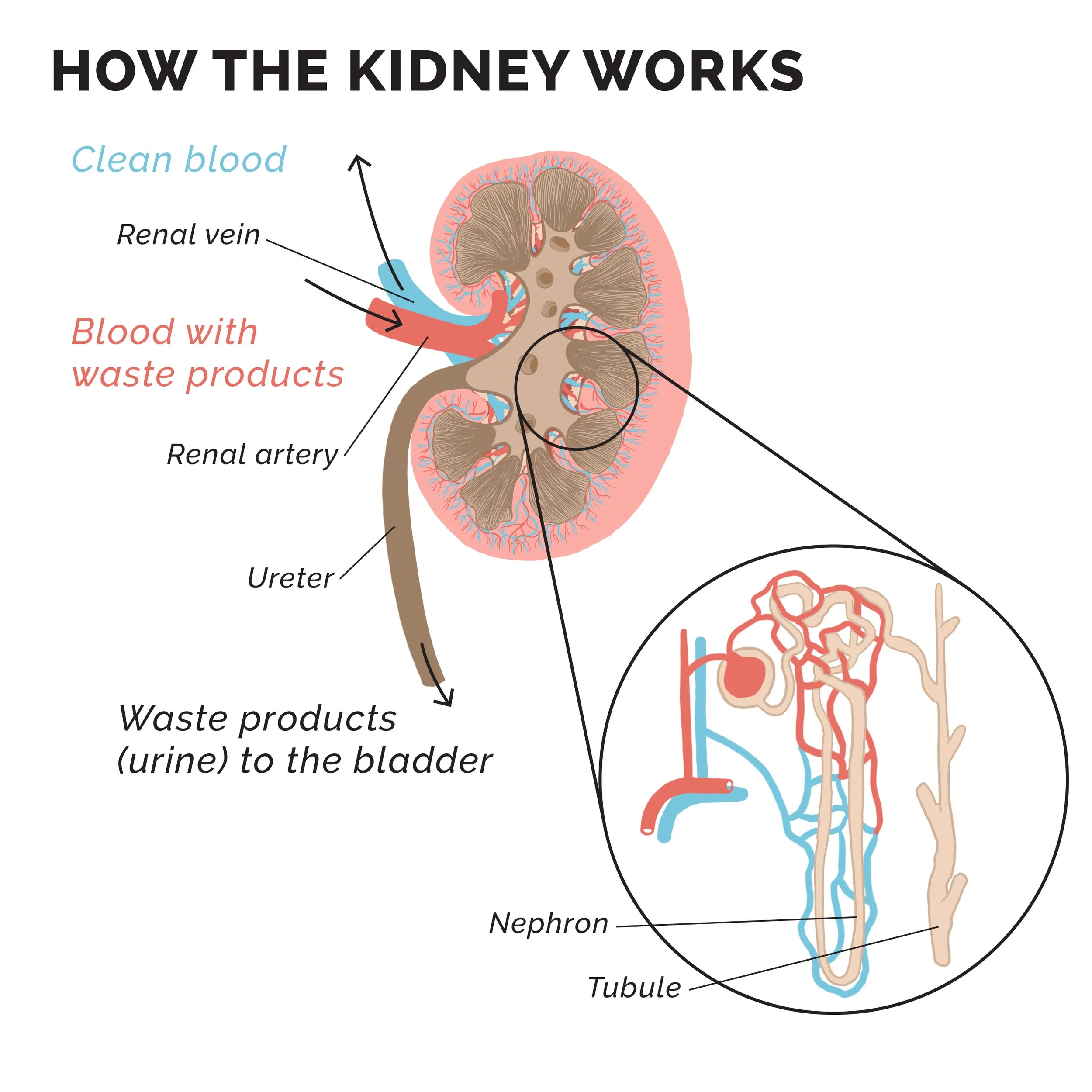
Mold toxins are considered mycotoxins. These compounds have activities that are harmful to humans, animals, and even other microorganisms. Their toxic nature includes neurotoxicity, nephrotoxicity, hepatotoxicity, immune dysregulation and suppressive properties, GI toxicity, cardio toxicity, carcinogenic, hematologic toxins, endocrine toxins, and more (2, 8).
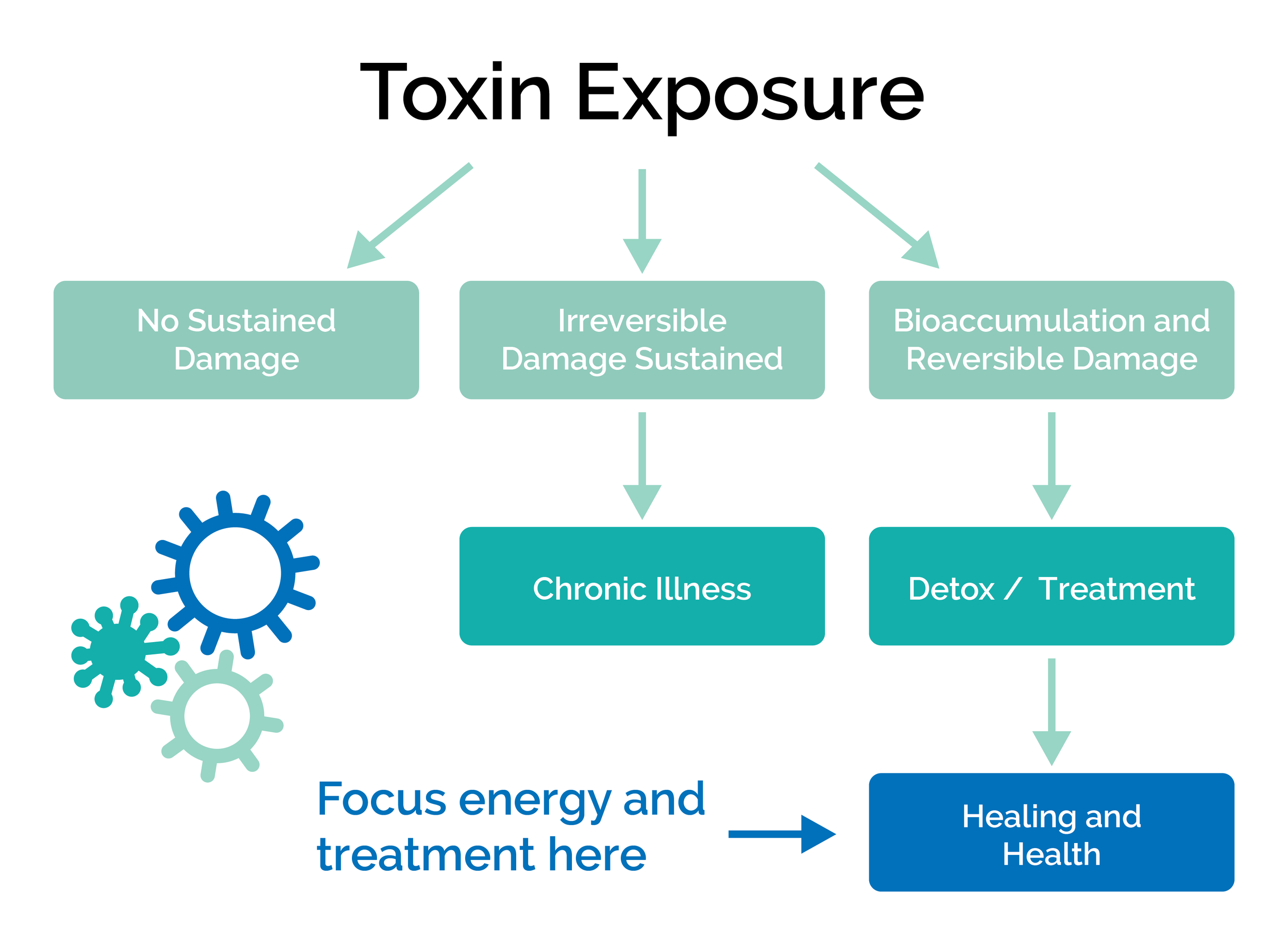
Myotoxicity has been referred to as the great masquerader in some scientific circles as it can present in many ways for different individuals. Exposure and symptomatology associated with mycotoxins is known as mycotoxicosis(2). It can be acute with a rapid onset that is clearly a large toxicity, or chronic which is a longer-term low-level exposure that usually results in cancers and more irreversible symptoms(2).
Myotoxicity differs from mold allergy due to the lack of an immune mediated response. The symptoms you may experience from toxins are due to the toxic nature that they already have. An allergy, on the other hand, is the body’s immunologic response mounted to protect us from a foreign substance. Symptoms arise due to the degranulation of mast cells and basophils and the release of chemicals like histamines(7).
This release is what causes allergic-like symptoms. In a pure toxicity state, you would not experience allergy symptoms. Also, someone without allergies could still feel the effect of mycotoxin overload, but wouldn’t suffer from congestion, itchy watery eyes etc. during allergy season. At least not from mold.
When people are going through a toxicity state they are often dealing with an active exposure. This exposure is less likely due to the outside air alone, but maybe experienced in high outdoor air exposure rates. During high mold spore count months (summer and fall) those who compost, garden, forage, or do other activities in the soil, toxicity can be seen from these activities and situations(5).
Though this is not what I commonly see. Water-damaged buildings and cars are the most common culprits for mold overexposure, in my experience. As said earlier, mold decomposes organic materials. Woods, wallpaper, and gypsum board are their fuel, due to the cellulose content, and happen to be extremely common building materials (1,5). When the mold is in ideal conditions it will grow in prominent levels and emit its toxic byproducts.
Mold Affects Each Person Differently
During large exposure levels toxicoses can occur. Various toxins can lead to different experiences, and individuality of people can lead to different manifestations. What does this mean? For example, you may have a stay-at-home mother and young child complaining of fatigue, anxiety, skin rash, ASD, GI issues etc., along with a partner and older child with no symptoms or mild fatigue or headache symptoms. Why is this?
Usually, in these cases the mother and child spend an exponentially greater time in the moldy home than the older child and partner. As they may be going out of the home for work/school. There are also four different, yet similar, genetic make ups that allow for or do not allow for adequate detoxification and may make them more susceptible to the toxin’s effects.
Situations also arise where the mold is concentrated in one person’s main living space that other family members do not frequent. Thus, increasing their exposure comparatively. All these factors are considered in mycotoxicosis. By understanding these differences and environmental spaces you can better pinpoint where the exposure is coming from.
Common toxic effects from mycotoxins include their ability to be neurotoxic, hepatotoxic, nephrotoxic, GI irritants, immune suppressant and modulating, skin irritants, hematologic toxins, carcinogenic, cardiovascular toxins, endocrine toxins, etc. due to the wide range of effects and the endless toxic profile someone could present with, the manifestations that can occur are also endless and look different in each person (2). Because of this, looking into mold toxicity would be a good place to start or to rule out for someone with a chronic disease or a new onset of symptoms.