On August 5-7, 2022, GPL Academy hosted the Mitochondria and Toxins: Advanced Strategies & Protocols in Chicago and live-streamed online. The following Q+A is a grouping of responses from the workshop presentations.
The material contained within this article is not intended to replace the services and/or medical advice of a licensed healthcare practitioner, nor is it meant to encourage diagnosis and treatment of disease. It is for educational purposes only. Any application of suggestions set forth in the following portions of this article is at the reader's discretion and sole risk. Implementation or experimentation with any supplements, herbs, dietary changes, medications, and/or lifestyle changes, etc., is done so at your sole risk and responsibility.

Joseph Pizzorno, N.D.
Joseph Pizzorno, ND is a world-leading authority on science-based natural medicine, a term he coined in 1978 as founding president of Bastyr University. A naturopathic physician, educator, researcher and expert spokesman, he is Editor-in-Chief of PubMed-indexed IMCJ, Chair of Board of IFM, board member of American Herbal Pharmacopeia, and a member of the science boards of the Hecht Foundation, Gateway for Cancer Research and Bioclinic Naturals. Author or co-author of six textbooks and 7 consumer books (Encyclopedia of Natural Medicine, The Toxin Solution), he has been an intellectual, political and academic leader in medicine for four decades.
Q: What was the supplement you recommended when using NAC for a patient?
A: N-acetylcysteine is readily available from many good companies. I use Natural Factors/Bioclinic Natural since I am a scientific consultant for them. I like adding fiber to help bind the toxins that NAC helps excrete.
Q: How do you detox arsenic? What nutrients or binders do you use to detox arsenic?
A: The best detox for arsenic is avoidance. Its half-life is typically 2-4 days, so avoidance is effective. The rate of detox can be increased by consuming dietary folates, not folic acid, and flavonoids such as phloretin.
Q: What are your thoughts on NAD and Glutathione IV therapy?
A: IV therapy can be helpful but should only be done by those who are very skilled and when the safer oral interventions are not adequate. Before giving anyone IV glutathione, be sure the blood is cleared of mercury.
Q: For someone with deletions in glutathione-S-transferase, what is the best way/form to increase GSH?
A: This is really two different issues. Glutathione-S-transferase uses glutathione, does not produce it. Oral NAC and liposomal glutathione increase GSH.
Q: With a sulfa allergy which is directly correlated with that deletion, is glutathione supplementation not recommended or cautioned?
A: I am not aware of sulfa allergy being a contraindication for glutathione.
Q: Is there any connection between the malate you are speaking about in your lecture and supplements with malate, such as calcium and magnesium malate?
A: Same molecule. Several minerals have been bound to Krebs cycle intermediates, supposedly to improve absorption and utilization.
Q: Do you have data on the effects of Metformin on Cplx 1 - causing acidosis?
A: Yes, Metformin does indeed cause pericellular acidosis. Anything which increases lactic acidosis causes acidosis, such as biguanides (metformin), antiretrovirals, statins, many more.

Elena Villanueva, D.C.
Dr. Elena Villanueva, producer and co-host of the 5 Part Series Mental Health Masterclass, the 5 Part Series Inflammation Masterclass, and The Leaky Brain Summit, is an internationally recognized crusader for ending the global chronic illness & mental health crisis by educating both the public and health professionals that mental health & other chronic illnesses are actually a body or brain health issue and not a disease. Elena has been featured on multiple occasions on FOX news, MSN, Healthline, Houston Chronicle, Anxiety and Depression Secrets Docu-Series, and several other documentaries. Dr Villanueva teaches on stages around the globe on evidence-based approaches for finding the underlying causes of chronic illness and brain-related conditions and how to use holistic and 'whole person' approaches to restore brain-related disorders and other chronic diseases.
Q: Do you have any experience with devices such as the NanoVi, to assist with mitochondrial function and proper folding of proteins?
A: I do not. I do however have experience with bioenergetics and how that shows improvement of mitochondrial function. In fact, a recent study was just completed by a university out of California showing the biological improvements in mitochondrial function and replication with the use of bioenergetics.
Q: What is your glyphosate protocol?
A: Glyphosate has a short half-life and is one of the toxins that can leave the body without help of added supplementation. However, the client must discover and stop his/her exposure to the glyphosate for levels to come down. When we detox, our protocols are designed to detox ALL toxins, chemical, myco, and HM’s… this simplifies the protocols (and reduces the costs) for patients/clients and makes them much more compliant and with that compliance you and your patients/clients will see more consistent positive outcomes.
Q: Are you concerned when toxins don't increase on testing between months 4-6 indicating they are not coming out as much?
A: Not as much of a concern as it is an indicator that the client/patient is not compliant with the protocols. By month 4-6, if they are compliant with reducing their exposure and taking their recommended supplements and food protocols, you will see one of the following two scenarios:
Their toxins will show higher indicating they are releasing toxins from their body
Their toxins will show lower because they have already released a good portion of their toxic load quickly.
If they are still showing the same levels after 3 months on deep detox, they are either still exposing themselves, not taking their protocols as recommended, or both. Keep in mind this is reflective for the protocols in our practice and may vary based on the protocols you establish.
Q: For a colonized fungal infection in the gut do you cycle, rotate, or use one over-the-counter anti-fungal at a time?
A: It depends. If the client/patient is not showing symptoms directly related to the fungal infection I focus instead on the broader picture with my deep detox protocols which also address fungal infections. If they are having considerable symptoms from the fungal infection, then yes, I put them on a fungal protocol first to mitigate their symptoms. Then I resume with my 12-month protocol system.
Q: I have a 34-year-old female with extreme CFS, ADHD and depression for 12 years. Organic Acids Test results are within normal limits except for borderline high arabinose and low Vitamin C. MycoTOX Profile results are positive for ochratoxin A, citrinin, and chaet (from previous home). Dealing with severe debilitating brain fog, memory issues, poor executive function. She wants to go back on Adderall but worried that it will affect mitochondria/adrenals. Any insight on the negative effects of psychostimulants on CFS?
A: We prefer to avoid those at all costs because of the negative side effects and potential damage they can have. If you are using effective protocols your client should be able to detox her mold toxins in an average of 9 months and you can include added brain and energy support during this time to help her… that could look like added high dose DHA, phospholipids, AA therapy, adrenal support, or even addressing vitamin and /or mineral deficiencies (according to labs) because those are common and can exacerbate brain fog, memory, etc.
Q: Can you comment on use of Vitamin D with Vitamin K? Why do you use Vitamin K?
A: High level overview on this: there are a percentage of people who have the VDR taq genetic variant and need Vitamin K to process their Vitamin D. Also, it simply ensures that the Vitamin D has the best chance at being utilized by the body. So, we are covering the bases without having to add more costly testing like genetic testing to their overall costs.
Q: Just wondering the rationale for doing just the methyl B12/folate vs. a good B complex with activated forms? How do they replete the other B vitamins if given just the folate and B12?
A: We do like using a good B complex with the methylated B12 and folate. However, at this time we have not found, nor have we been able to formulate a B complex that has the high therapeutic grade doses of methyl B12 methyl folate we prefer to use… therefore we use just the Methyl B12 and Methyl folate that we created in our brand at BioOne Sciences. There are some clients that we will put on additional B Complex. And all our clients that go into a year 2 program with us (which is most of them), get switched over to a B Complex (with the methylated B12 and Folate). We haven’t had an issue with repletion of the other B’s.
Q: Could we get your pdf form for patients to record their lab results and significance?
A: Please reach out to us at info@modernholistichealth.com We will be emailing our practitioners who are interested in learning our systems with information on our first live, in person training that we want to do and from that training we will share all our forms and protocols with you.
Q: What is in your tox bundle? OAT, MycoTOX Profile, Heavy Metals and what else?
A: Yes, those plus the environmental toxins and Glyphosate.
Q: What was the biofilm agent you said you used?
A: It’s our TCG Activation product that is humic/fulvic based.
Q: Is it normal for a patient to get full body edema during a detox?
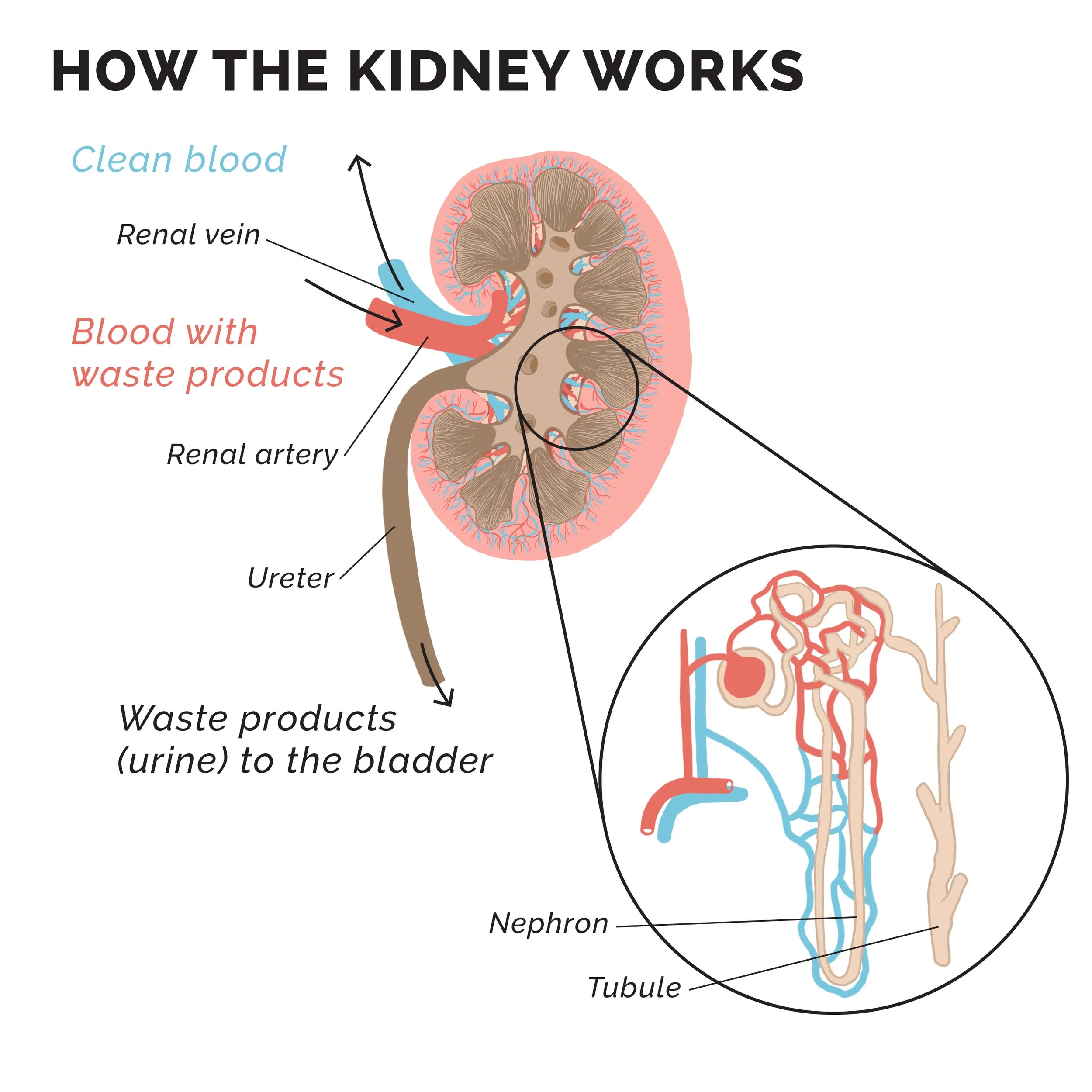
A: No, it is not normal. It sounds like their detox pathways are not open and you should have your patient stop immediately. Be sure you check their blood labs for kidney and liver function, make sure they are having full evacuation bowel movements, and check for methylation challenges with some genetic testing. You might also get a history on any issues with their lymphatic system as well and determine if they have any allergies or sensitivities to any of the ingredients in the supplements you have them on.

LEARN NEW WAYS TO HELP PATIENTS WITH DIFFICULT-TO-DIAGNOSE AND CHRONIC HEALTH ISSUES.
The tests discussed throughout each workshop are all used to help identify exposure sources and biochemical imbalances in individuals with chronic health conditions. The Organic Acids Test (OAT) contains multiple markers which may be influenced by environmental and mold toxins. Often, the combination of the OAT, MycoTOX Profile, and GPL-TOX Profile can be used to help identify how a patient might be getting exposed, as well as assist with correlating their symptoms back to these sources. Determining the underlying causes of chronic illnesses for patients is the key to integrative medicine, not just treating the symptoms. The Great Plains Laboratory continues to find new ways to detect these causes of many illnesses and study the correlations between the results and conditions.
Registration includes:
Ability to purchase GPL tests discussed throughout the program at special workshop-only discounted rates.
60-day access to the full conference recordings.
Permanent PDF access to each speaker’s slides.
The option to purchase continuing education credits (5 credits per day), whether you attend in-person, watch Live Online, or watch the conference recordings at a later date! See detailed information about credits.
An interactive Workshop Hub website where you can live chat and network with attendees and ask questions to the speakers.
And last, but most certainly not least, qualified practitioners will receive a free OAT.